
Lower back pain stands as one of the most prevalent musculoskeletal complaints yet most people have been sold an incomplete solution. They’re offered machines, injections, and prolonged rest when what their body needs is precision manual therapy from a registered physiotherapist or chiropractor.
The human spine is a mechanical marvel, but it operates on principles that no ultrasound machine or heating pad can fully address. Your lumbar region houses a complex network of joints, ligaments, muscles, and neural pathways. When something goes wrong—and lower back pain tells you something has gone wrong—the solution must address the underlying mechanical dysfunction. That’s where manual therapy becomes non-negotiable.
This clinical guide breaks down exactly what causes lower back pain, what it means when you’re experiencing it, and why hands-on treatment remains the most direct path to durable recovery.

What Is Lower Back Pain, Really?
Lower back pain is not a single condition. It’s a symptom that reflects dysfunction somewhere in your lumbar spine (L1 through L5), the supporting musculature, or the neural structures passing through the region.
Here’s what matters clinically: pain location tells a story. Pain centered at your L4-L5 disc differs from pain radiating into the glute, which differs from stiffness that worsens with forward bending. Each pattern points to a specific tissue problem—and each demands a different therapeutic approach.
The three most common mechanical origins:
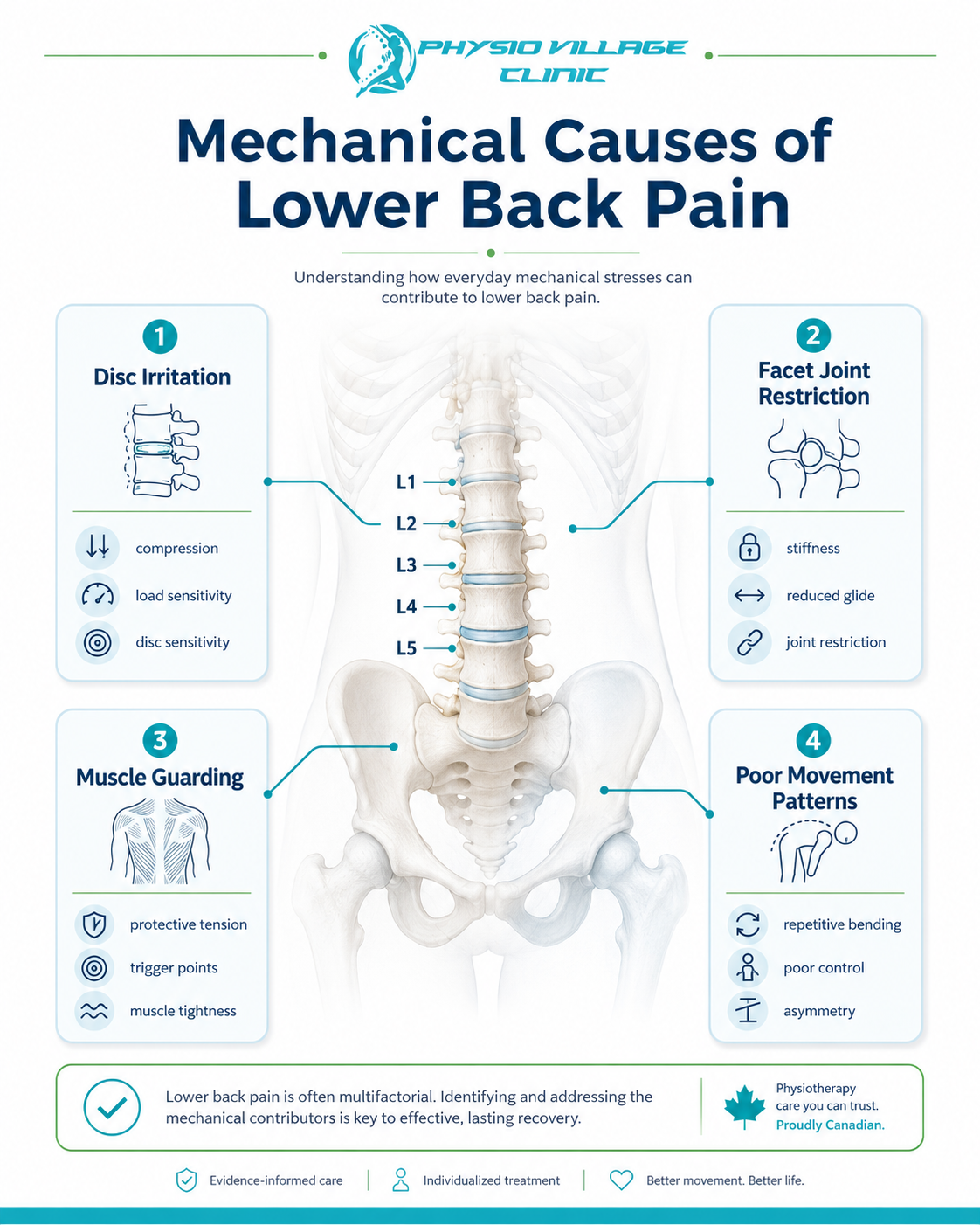
Your intervertebral discs may have lost hydration or developed a small tear. The facet joints (where vertebrae meet) might be irritated or slightly misaligned. Muscular guarding—your deep stabilizers working overtime—can create a pain cycle that perpetuates itself. A skilled manual therapist assesses which of these (or what combination) is driving your symptoms.
Back Pain Causes: The Mechanical Truth
Postural Dysfunction and Daily Movement Patterns
Most people sitting in modern office environments don’t maintain neutral spine posture. Over months and years, this creates asymmetrical loading across your lumbar discs and facet joints. The problem isn’t the position itself—it’s the static repetition without countermovement.
Manual therapy addresses this by restoring joint mobility and teaching your neuromuscular system what neutral actually feels like. A physiotherapist can mobilize restricted segments and release hypertonicity in your hip flexors, which directly alters spinal loading mechanics.
Disc-Related Dysfunction
Your intervertebral discs act as shock absorbers and load distributors. When they lose hydration—which happens with prolonged static postures, dehydration, or age—they become less resilient. A disc bulge or early herniation can irritate nerve roots or simply create mechanical pain through inflammatory response.
Here’s the clinical insight: disc pathology on imaging doesn’t always correlate with pain severity. Two people with identical MRI findings can have vastly different symptoms. Why? Because manual therapy can restore the mechanical environment such that the disc is no longer irritated, regardless of the morphology visible on scan.
Mobilizing the spine to improve segmental motion, releasing muscular tension that’s compressing the disc, and correcting movement patterns all reduce mechanical irritation—often within 4-6 weeks of consistent hands-on treatment.
Muscular Stabilization Failure
Your core isn’t your six-pack. Your true core includes your transverse abdominis, multifidus, diaphragm, and pelvic floor—all working together to maintain spinal stability. When these muscles fail to activate properly (often due to pain inhibition or neural dampening), your spine becomes mechanically unstable.
This instability forces your superficial muscles—your rectus abdominis and erector spinae—to work overtime, creating chronic tension and fatigue. Manual therapy combined with motor control retraining restores this deep stabilization pattern. A registered physiotherapist assesses which segments lack stability and prescribes precision exercises to restore neuromuscular control.
Facet Joint Irritation
Your facet joints are small but critical articulations between adjacent vertebrae. They guide spinal motion and share load-bearing responsibility with your discs. When they become irritated through overuse, misalignment, or age-related changes, they refer pain into the low back and sometimes into the buttock.
Manual mobilization of restricted facet joints—performed by a trained chiropractor or physiotherapist—can immediately improve joint mechanics and reduce irritation. This is hands-on therapy working at its best: directly addressing the dysfunctional joint rather than medicating symptoms.
The Difference Manual Therapy Makes
Machines cannot assess the subtle restrictions in your spinal segments. They cannot feel whether your L4-L5 facet is compressed or whether your lumbar multifidus is inhibited from pain. They cannot restore proprioception or retrain neural pathways. A registered physiotherapist can do all of this in a single session.
Hands-on interventions that matter:
Spinal mobilization restores segmental motion and reduces mechanical irritation. Soft tissue release targets muscular guarding patterns that perpetuate pain cycles. Joint mobilization improves facet joint mechanics and loading patterns. Myofascial release addresses fascial restrictions that limit mobility and create referred pain patterns.
These techniques work because they address tissue-level dysfunction, not just symptoms. When your physiotherapist mobilizes a restricted segment, the neurophysiological response is immediate: proprioceptive input normalizes, pain gates begin to close, and movement becomes easier. This is why manual therapy often provides relief within the first 2-4 sessions—you’re restoring mechanical function.
Technology has a role—shockwave therapy can stimulate healing in tendon attachments, for example—but it amplifies the effect of manual therapy rather than replacing it. A joint that has been properly mobilized and stabilized responds far better to any adjunct modality.
Symptoms: When You Should Seek Immediate Care
Local lumbar pain (centered in your lower back, worse with certain movements) typically responds excellently to manual therapy. The mechanical nature of the problem means manual assessment can identify and address it directly.
Radicular pain (pain traveling down one leg, often with numbness or tingling) suggests nerve root irritation. This requires a thorough assessment to rule out serious pathology, but when cleared, manual therapy—specifically nerve mobilization techniques—can be transformative. A physiotherapist trained in nerve gliding exercises can restore nerve mobility and reduce the irritation creating your symptoms.
Stiffness and reduced mobility, especially on one side or with specific directions of movement, tells you that joint restriction exists. This is where manual therapy excels. A few sessions of skilled mobilization often restore near-normal mobility.
Red flags requiring immediate medical evaluation:
- Sudden loss of bowel or bladder control
- Progressive neurological deficits (worsening weakness or numbness)
- Fever with back pain
- Pain following trauma with signs of fracture
- Night pain that wakes you repeatedly
If you’re experiencing any of these, seek emergency assessment before physiotherapy. Physio Village’s registered practitioners are trained to screen for these patterns and refer appropriately.
Evidence-Based Lower Back Pain Relief Strategies
Phase 1: Acute Management (Weeks 1-2)
Your first priority is pain reduction and mobility restoration. A registered physiotherapist will:
- Assess the mechanical nature of your problem through hands-on testing
- Apply manual mobilization to restricted segments
- Use soft tissue release to reduce muscular guarding
- Prescribe 2-3 pain-reducing exercises you can perform at home
This phase typically requires 2-3 sessions weekly. Manual intervention directly reduces pain through mechanical and neurophysiological pathways—you’ll feel meaningful improvement within the first week.
Phase 2: Stabilization and Retraining (Weeks 3-6)
Once acute pain begins to resolve, the focus shifts. Your physio will:
- Introduce precision core stabilization exercises targeting your deep stabilizers
- Progress to functional movement patterns that replicate your daily activities
- Continue manual therapy to maintain mobility gains and address residual restrictions
- Teach you to recognize and self-correct movement patterns that initially created the problem
This is where lasting recovery happens. Many people stop attending once acute pain resolves, then relapse months later when they encounter a similar movement pattern. Completing this phase prevents recurrence.
Phase 3: Return to Function (Weeks 7+)
Progressive loading, sport-specific or work-specific training, and independent self-management become the focus. Your physiotherapist ensures you can tolerate your desired activities without regression.
Why Manual Therapy Outperforms the Machine-Only Approach
Here’s what the clinical evidence shows: manual therapy combined with exercise produces superior outcomes compared to exercise alone, machines alone, or passive modalities alone. The human hand provides diagnostic information and therapeutic specificity that no machine can match.
A registered physiotherapist assesses whether your restriction is due to joint stiffness, muscle guarding, fascial adhesion, or neural tension—then applies the specific manual technique addressing that exact problem. This precision matters. A mobilization that’s slightly misaligned in direction or amplitude is ineffective. A physiotherapist adjusts based on real-time tissue feedback.
Machines deliver consistent force but lack adaptive intelligence. A patient experiencing acute guarding needs gentler mobilization; a patient with chronic stiffness needs progressive loading. A skilled manual therapist reads these patterns and adjusts treatment in real-time.
What to Expect at Physio Village
At our Oakville clinic, your first appointment involves a comprehensive assessment. Your physiotherapist will:
- Take a detailed history of your pain onset, pattern, and aggravating factors
- Perform orthopedic testing to identify the mechanical dysfunction
- Assess your movement patterns and postural habits
- Palpate your lumbar spine to assess mobility and identify areas of restriction
- Screen for serious pathology and refer if indicated
Following this assessment, your physio will perform hands-on treatment addressing the identified dysfunction. You’ll feel the difference immediately. We’ll also provide 2-3 specific exercises to perform daily at home.
Your treatment frequency depends on severity—typically 2-3 times weekly initially, reducing to 1x weekly as you progress. Most mechanical lower back pain improves substantially within 4-6 weeks of consistent manual therapy and prescribed exercise.
The Self-Assessment: Can You Identify Your Pattern?
Try this simple mobility check:
Stand upright. Slowly bend forward from your hips, allowing your arms to hang. Note where you feel restriction or pain:
- Pain at the center of your lower back with forward bending suggests discogenic pain or facet irritation. This pattern often responds exceptionally well to manual therapy.
- Pain on one side only, worse with forward bending suggests unilateral facet irritation or muscular guarding on that side.
- Pulling sensation in the back of your thigh or into your buttock suggests hamstring tightness or potential nerve root irritation.
- Sharp pain with any movement warrants a professional assessment to rule out acute injury.
If you’re unable to bend forward 60-70 degrees without significant restriction or pain, mobility impairment exists. This is exactly what manual therapy addresses most effectively.
Lifestyle Integration: Supporting Your Recovery
Manual therapy provides the mechanical reset. Your behaviour maintains it.
Sleep positioning: Your lumbar spine should maintain its natural curve. Side sleepers should place a pillow between their knees. Back sleepers should place a pillow under their knees. Avoid prone sleeping when possible.
Daily posture: Every 30-45 minutes at a desk, stand and walk for 2-3 minutes. Your disc hydration depends on movement and unloading. Prolonged static posture—even good posture—creates problems.
Hydration: Your discs lose water with dehydration. Adequate fluid intake (2-3 litres daily) supports disc hydration and overall disc health.
Movement variability: The worst posture is the one you maintain for hours. Vary your positions. Sit, stand, move. Your spine evolved for motion, not stasis.
Strength maintenance: Once your physio has cleared you to progress, continue the exercises you’ve learned. Your core doesn’t go back to baseline—it requires ongoing activation to remain stable.
Questions You Should Ask Your Physiotherapist
- “Based on your assessment, which structure do you believe is primarily driving my pain?” (They should give you a specific answer: disc, facet, muscle, nerve.)
- “How many sessions do you estimate until I return to normal function?” (Honest physios give realistic timelines: usually 4-8 weeks for mechanical lower back pain.)
- “What happens if I plateau? What’s your plan to progress further?” (Good clinicians have contingency strategies.)
- “Can you teach me the movement patterns to prevent this from recurring?” (This is the critical distinction between temporary relief and lasting recovery.)

Key Takeaways: Your Path Forward
Lower back pain is mechanical dysfunction, and mechanical dysfunction responds to hands-on diagnosis and treatment. Machines cannot provide this. Rest without directed therapy prolongs recovery. Continued movement patterns that created the problem will perpetuate it.
A registered physiotherapist or chiropractor trained in manual therapy can assess your specific mechanical problem, address it through skilled hands-on intervention, and teach you to prevent recurrence. This is clinical. This is evidence-based. This is the fastest path to durable recovery.
Your lower back pain has a cause. Find that cause. Address it mechanically. Recover completely.
Clinical Action Plan
This week: Contact Physio Village for your initial assessment. Bring any recent imaging (MRI, X-rays) if available.
Your assessment appointment: Your physio will identify the mechanical dysfunction driving your pain. You’ll receive manual treatment and 2-3 therapeutic exercises.
First 4 weeks: Attend 2-3 sessions weekly. Perform prescribed exercises daily. Your pain should reduce substantially and function should improve measurably.
Weeks 5-8: Progress to 1x weekly sessions as you transition to independent self-management and return to your desired activities.
Ongoing: Maintain the movement patterns and exercises your physio has taught you. Your spine requires continued activation to remain stable and pain-free.
Connect With Our Clinical Team
Do you know someone in Oakville or Brampton struggling with lower back pain? Share this clinical guide to help them understand their options. Many people suffer with lower back pain for months or years without realizing that a registered physiotherapist can assess and address the mechanical problem directly.
Try this simple mobility check: Stand upright and slowly bend forward, letting your arms hang. If you can’t reach your knees without significant restriction or pain, mobility impairment exists. This is exactly what manual therapy addresses most effectively. Perform this check weekly during your recovery—it’s your objective measure of progress.
Book Your Assessment
Oakville Clinic: Book Oakville Clinic
Brampton Clinic: Book Brampton Clinic
Your lower back pain has a cause. Manual therapy can find it and fix it. Schedule your comprehensive assessment with a registered physiotherapist today.


